 Saibe Fulya Elmastaş Akkuş1 , Sevda Şener Cömert1 , Erdem Emre Gülşen2 , Hasibe Çiğdem Erten1 , Ali Fidan1 , Nesrin Kıral1 , Esra Kılıç3
Saibe Fulya Elmastaş Akkuş1 , Sevda Şener Cömert1 , Erdem Emre Gülşen2 , Hasibe Çiğdem Erten1 , Ali Fidan1 , Nesrin Kıral1 , Esra Kılıç3 2Department of Pulmonology, Dr. Mustafa Kalemli Tavsanlı State Hospital, Kütahya, Türkiye
3Department of Pulmonology, Sultanbeyli State Hospital, İstanbul, Türkiye

Abstract
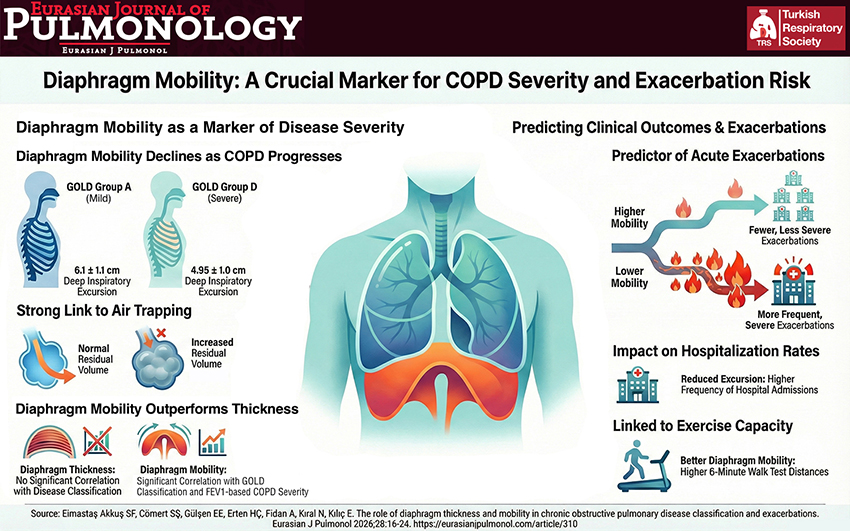
BACKGROUND AND AIM: Chronic obstructive pulmonary disease (COPD) is a systemic condition. Oxidative stress and air trapping may lead to alterations in diaphragm mobility and thickness. Therefore, assessing diaphragm function in these patients is of great importance. The aim of this study is to evaluate diaphragm thickness and mobility using ultrasonography in COPD patients and to determine their relationship with clinical classification and exacerbation frequency.
METHODS: This single-center, prospective study assessed diaphragm excursion, diaphragm thickness, inspiratory and expiratory durations, contraction speed, and thickening fraction using ultrasound. Spirometry and diffusing capacity for carbon monoxide were performed, and lung volumes and capacities were calculated. Patients were followed for three months to record the number and severity of exacerbations and hospitalizations. Diaphragm parameters were compared with clinical and functional tests to examine their association with COPD classification and exacerbations.
RESULTS: A total of 81 patients, 70 of whom were male, were included in the study. Diaphragm excursion during deep inspiration showed a significant negative correlation with FEV1 classification (r=-0.38, p<0.001). Significant correlations were also observed between diaphragm excursion during deep inspiration and residual volume (RV) (%; L) (r=-0.39, p<0.001; r=-0.37, p<0.001) and the residual volume/total lung capacity ratio (RV/TLC) (r=-0.52, p<0.01). Diaphragm excursion during deep inspiration significantly decreased with increasing Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage (p=0.007). No significant differences were found between
diaphragm thickness and either GOLD or FEV1 classification. During the three-month follow-up, patients with lower diaphragm excursion during deep inspiration experienced significantly more exacerbations (p=0.012).
CONCLUSIONS: Our study demonstrated that diaphragmatic excursion during deep inspiration is associated with GOLD classification, FEV1 severity, and the frequency of acute exacerbations. Our findings suggest that diaphragmatic dysfunction in this context is more closely related to impaired mobility than to reduced muscle thickness. Although diaphragmatic excursion was significantly associated with exacerbation risk in univariate analysis, it did not remain an independent predictor after multivariable adjustment. Further longitudinal studies are warranted to better define the prognostic significance of diaphragmatic excursion in COPD.
Graphical Abstract